 |
| Image from Lipoedema Australia Support Society (LASS) |
In lipedema (also spelled lipoedema), the fat cells in certain parts of the body experience overgrowth. It results in an abnormal accumulation of fat, particularly in the lower half of the body; often the arms are affected too. This can affect the efficient flow of lymph as the condition progresses.
As we have discussed, lipedema is rarely recognized by doctors, despite being discovered 75 years ago. Often it is thought to be simple obesity, or it is confused with lymphedema, the accumulation of lymph fluid in the interstitial areas, since secondary lymphedema can develop in the later stages of lipedema.
In Part One of this series, we discussed the typical features of lipedema and how differentiate between lipedema and lymphedema.
In Part Two of the series, we discussed how lipedema progresses, the different stages of progression, and why it's so important to be aware of lipedema
In Part Three of the series, we discussed the different types of fat distribution patterns, looked at some pictures to illustrate type and stage of lipedema, and detailed how lipedema is diagnosed.
In Part Four of this series, we examined possible causes of lipedema, as well as medical conditions often associated with it.
Now, in Part Five, we will discuss possible treatments for lipedema in detail. Because we want to give more detail about each option, we are breaking the treatments into several sub-posts:
- Traditional Medicine Treatments
- "Weight Control" and Special Nutritional Approaches (trigger warning)
- Tumescent Liposuction
- Alternative Medicine Treatments
Today, we are talking about the controversial topic of "Weight Control" and Special Nutritional Approaches for treating lipedema.
Caveats and Trigger Warning
Many larger people are ignorant of lipedema or have questions about it but avoid lipedema sites because of weight loss talk or body negativity. My aim is to create a lipedema resource that is more size-friendly in order to raise awareness of this condition. However, not everyone defines "size-friendly" in the same way.
After years of dieting and eating-disordered behaviors, some find any mention of diets, weight loss, or bariatric surgery triggering. Others simply don't find those choices compatible with body love or Health At Every Size®. Unfortunately, because "weight control" is such a common prescription for lipedema, treatment discussions have to have at least some discussion of those topics. Here's how I plan to address them.
Weight loss or "weight control" is often pushed for lipedema patients, so we will discuss the evidence for such recommendations. Although I personally oppose bariatric surgery, the reality is that many women with lipedema consider it or are pressured towards it, so the pros and cons of bariatric surgery for lipedema will also be discussed. Special nutritional diets are also often prescribed, so we will discuss whether these can be used to lessen the symptoms of lipedema. In addition, The Health At Every Size® paradigm will be discussed as an alternative to weight-centric approaches.
While many lipedema websites are biased towards weight loss or diet-like behaviors, my own bias is the opposite way ─ against dieting, weight loss surgery (WLS), and rigid nutritional protocols. Readers should know that my viewpoint will show in this post.
However, people always have the right to make their own healthcare decisions, so people who choose weight loss or WLS are absolutely welcome here. Please don't feel put down if you choose these options. But do understand that diet talk is very triggering to some and they deserve a safe space away from it. Please respect the mission of the blog and do not promote WLS or engage in diet talk or negativity here. There are plenty of other sites for discussing those choices; this is not one of them.
My goal is a "size-neutral" approach to Lipedema. I will not promote bariatric surgery, weight loss, or a particular nutritional approach, but I will give information about all the commonly-prescribed treatment options, including those I wouldn't personally choose. This is your choice, and you are trusted to be smart enough to research and pursue the treatment that seems right for YOU. Please extend compassion, empathy, and respect for the right to make individual health choices to others and monitor your comments accordingly.
Trigger Warning: Weight loss, weight control, weight loss surgery, and various nutritional approaches are discussed as possible treatments for lipedema.
Introduction
Because many people with lipedema are quite heavy, lipedema is usually mistaken as "just" obesity. Many women tell the story of how their concerns were brushed off and they were told to just go and lose weight, even when they insisted that something else was going on:
- I was always told to lose weight by GP's. A friend in England...had Lipoedema and she told me I had it. It took 8 years to get a medical diagnosis
- First three attempts, I was smiled at patronizingly, not examined and given leaflets on dieting…I tried again with a different GP, who also refused to examine me and said, "Face facts, you're FAT. Stop wasting my time and yours and go to a gym"…I still have problems as when I explain to healthcare professionals in hospitals that I have lipoedema, they act as if I'm so far in denial that I'm 'fat', I've 'made up' a condition to explain it
- I spent 16 years going from doctor to doctor in Eastern Idaho, trying to find out what was wrong with my legs. Some said lymphedema and some said I was just fat. After I got the diagnosis from the Mayo Clinic I tried explaining to my doctors about lipoedema but they weren't very interested; [since] there wasn't even a diagnosis code for it they couldn't accept it as a valid condition
Even when doctors accept that lipedema is a real condition, they often still blame its severity on being fat or on "bad" habits. Yet lipedema is a disorder whose main symptom happens to be overgrowth of fat tissues. Obesity occurs as a result of lipedema, but it does not cause it. As one British organization notes:
Obesity frequently occurs as a result of this condition, and not the other way around. It is important to realise that you have not caused your Lipoedema by poor dietary issues or from being overweight.Because it is so common to blame lipedema on lack of self-control, there is a long history of using weight management techniques to control it. These are not very effective, but many providers remain adamant that weight management must remain a central part of treating lipedema. Weight bias is alive and well, even among lipedema providers who ought to know better, and it influences the treatment advice many women are given.
The topics of weight loss, bariatric surgery, weight control, and special nutritional approaches are controversial ones within the lipedema community. Some women believe wholeheartedly in weight loss, some oppose it, and most fall somewhere in between. Most doctors admit that dieting is not effective for lipedemic fat ─ but then turn around and give patients strict dietary regimes for "weight control" or push bariatric surgery. Others strongly promote particular nutritional approaches ─ supposedly just to ease symptoms or prevent further weight gain ─ but with the judgmental language of diet doctors.
Let's look at the evidence for each of these choices a bit more closely, as well as how weight bias has influenced these recommendations.
Weight Loss for Lipedema
For many years, women with lipedema were told to just lose weight and their legs would normalize. What was the evidence for this recommendation? NOTHING. A 2013 study notes:
There have been no published trials reporting weight management in lipoedema.NO trials. Zero, zip, nada, NOTHING. Doctors just assumed that weight loss would help lipedemic legs, but there is no proof that it does.
With no research on it, doctors describing the condition of lipedema relied on their own observations and the anecdotal reports of women who had lipedema. From the original studies on lipedema on, women uniformly told doctors that weight loss did not significantly reduce their leg size. This was consistent with what most doctors saw in their lipedema patients.
Consequently, most medical literature acknowledges that stringent diets produce little weight loss from the lower half of the body in people with lipedema, even though there is little proof one way or the other. One resource notes:
Because it is not a medical condition caused by over-eating and improper nutrition habits, diets will not [have] much of an effect.Even so, weight loss is still a commonly-prescribed treatment, even from lipedema experts. A textbook by one of the pioneers in the lipedema field says:
In the combination form, lipedema-plus-obesity, it is essential that the [Complete Decongestive Therapy] be accompanied by a professionally supervised weight-reduction program.Doctors who recommend weight loss for lipedema are hoping against hope that it might produce some limb reduction in the lower body or prevent the development of secondary lymphedema. Others simply don't believe that lipedemic women have "tried hard enough" or used the "right program" to lose weight.
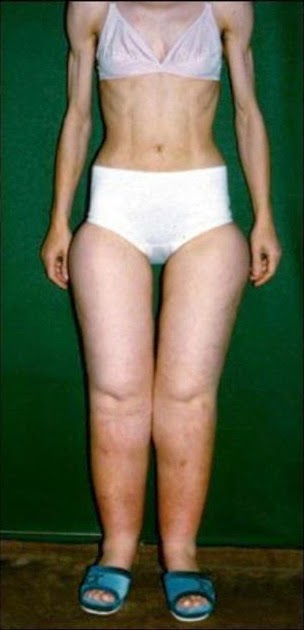 |
| Anorexic patient with lipedema |
There are even cases of lipedema in women with anorexia, like the woman pictured. This woman has dieted herself into anorexia on top, but her legs are still fat.
Another woman shared her experience with anorexia and lipedema in a recent news report. She said, "I put myself on a super strict-caloric diet and you could see my rib cage, you could see my ribs, my face was gaunt, my hands were just sticks, but my legs and my arms were still big."
Yet still providers keep pushing weight loss in women with lipedema. They have been trained to see weight loss as the only "correct" response to a fat body and that this message cannot be eased up on at all.
Indeed, the 2013 study discussed above challenged the notion that weight cannot be lost on the lower body of lipedema patients. It triumphantly noted modest limb reduction in one patient with lipedema after 18 months of dieting; she lost about 22 lbs. and about 14% of total limb volume. The study concluded, "The case study presented in this article shows that, by addressing generalised obesity, leg size in the person with lipoedema can be reduced."
This kind of sweeping generalization is typical overstatement. 18 months in ONE patient is hardly proof. Many people see weight reductions from dieting on this timeline, only to see that weight return within another year or two after that. And a case report of ONE patient is far from conclusive that weight loss is helpful for lipedema.
But surely some women with lipedema lose weight successfully? Yes, occasional stories can be found online of restrictive dieting (without WLS) producing significant weight loss, including modest reduction in affected areas.

Here is a picture of a woman who lost over 100 lbs. and re-shaped her upper body through exercise, but who clearly still has significant lipedema in the legs. Her legs have probably had some volume reduction, but remain disproportionately larger despite strict diet and exercise.
And, as with most weight loss, weight loss in lipedemics usually does not last. Even those women with lipedema weight loss "success" often experience regains. So are a few anecdotal stories really proof that weight loss is the treatment of choice for lipedema?
Bottom line, there is little long-term, qualitative research on weight loss for lipedema. Doctors just assume it will help but have little real data to support that. Any recommendation for weight loss as treatment is not an evidence-based recommendation.
Again, anecdotal evidence suggests that weight loss may provide some short-term reduction in limb volume in some, but legs almost never reach "normal" proportions. Rarely does weight loss seem to provide long-term help; limb volume tends to return with time.
Dr. Karen Herbst, a leading lipedema researcher, says:
Lifestyle improvements should always be considered but are not the cause of lipedema. Lipedema SAT [Subcutaneous Adipose Tissue] is unaffected by caloric restriction alone.Doctors who continue to recommend weight loss for lipedema are doing so mostly from weight bias, because that's what their medical training tells them to do with a fat body, and because they don't know what else to recommend. One woman with lipedema writes:
If you are struggling with your weight [because of lipedema] and you cannot lose and you've tried everything, don't let your doctor convince you that you aren't trying hard enough.Lipedema is not about calories in and calories out, and weight loss is not a cure for lipedema. Calories are not irrelevant, but this is a disease of adipose overgrowth. That disease process means it's very unlikely that you can make your body look "normal" no matter how hard you try.
Even knowing that weight loss attempts are unlikely to "normalize" your body size and shape, can you still choose to pursue it? Of course you can, and many women with lipedema do. Everyone is the boss of their own body, and if this is the path you want, it's your right to pursue it. But it's important to be realistic about it. Even the most successful weight loss programs usually only produce about a 3-5% loss long-term for most of their participants. Some do lose more, but the majority only lose a small percentage of their total weight.
There's nothing wrong with an emphasis on healthy, reasonable eating, and exercise is very important for lipedema patients. How you eat can absolutely influence your body, but the reality with lipedema is that you only have so much control over it. Sometimes gains occur despite your best efforts, and sometimes you just don't lose much weight. Do your best and don't beat yourself up over it.
Don't let the misguided weight bias of doctors push you into harmful dieting practices or into feeling like a failure because you don't have a skinny body. Lipedema is NOT your fault. Let go of the guilt and find a new, rational way of dealing with your body.
Weight Loss Surgery for Lipedema
 |
| Image from lipedemasimplified.com |
Many doctors push WLS, especially gastric bypass, for women with severe lipedema. In addition, many women who don't know they have lipedema opt for WLS in a last-ditch attempt to lose weight when nothing else is working.
But before addressing WLS, the real question here is why are so many women with lipedema quite fat? The answer is that severe lipedema predisposes to large weight gains, even when the person is working hard against these gains.
Some resources call these sudden gains "inflammatory cascades." I prefer the term "flares" because we don't have any real proof yet that inflammation is the cause. Most Stage 3 lipedemic women have experienced "flares."
No one knows why some women are so prone to flares while others stay fairly stable or progress more slowly. Doctors like to believe that severe gains happen only in those patients with terrible eating habits or a binge eating disorder on top of the lipedema. But women's stories suggest the truth is more complicated.
Sometimes women gain very large amounts in relatively short periods of time, so much that it is difficult to believe that it could be due simply to overeating. One woman gained over 350 lbs. in the space of a little over two years. How could someone eat enough to gain that much weight in that amount of time? Even with a significant binge habit, it would be difficult. More likely, there's a lipedema flare and endocrine issues going on.
And in fact, the woman involved reports that she had the triple-whammy combination of hypothyroidism, PCOS, and lipedema. This resulted in a severe case of lipo-lymphedema.
[Personally, I gained about 100 lbs. over the period of about 3 years due to the same triple-whammy, despite desperate attempts to stop it with stringent diet and exercise.]
Some of this severe weight gain is fluids, other parts are fat. If fluids are not mobilized, much of the extra weight may become permanent. This can lead to many health problems. And the combination of extra weight and lipedema's predisposition to joint issues can lead to major mobility issues.
As a result, a number of women with severe lipedema resort to bariatric surgery, and some lipedema providers promote bariatric surgery for their "obese" lipedemic patients. Although experience shows that WLS will not give lipedema women a "normal-sized" lower body, they hope that there will be reduction in the size of affected areas and an easing of lymphedema. They also hope that by reducing their overall weight elsewhere, some of the strain will be taken off of their legs and health co-morbidities might be lessened.
And who could blame them for this hope? It seems logical on the surface, and certainly severe lipo-lymphedema is a tremendous physical burden with many health implications. Any relief of even part of this burden seems very enticing indeed.
Unfortunately, there is little data to support or refute whether bariatric surgery is a good choice for lipedema patients. Mostly we have only anecdotal stories, usually from those who have had success with this approach; those who don't rarely publicize their journeys, especially when they experience serious side effects and complications from the surgery. And even the ones who are successful at first often experience significant weight regain in a few years. The pressure not to speak up about negative outcomes and weight regain is very strong in the WLS community, so this side of the story is often not heard as loudly as the success side.
The anecdotal stories I've found suggest that WLS is somewhat helpful to some degree for some women, mostly those with very significant lipo-lymphedema who also get concurrent treatment for lymphedema. Weight and size in lipedemic areas is lost, but the body remains significantly disproportionate. Co-morbidities like diabetes tend to lessen, at least for a while, and mobility usually improves. These are significant advantages.
However, people must be realistic about the risks of this option. If not done carefully, operations of any kind can damage the lymph system further and result in serious complications. Furthermore, many people experience major nutritional deficits after malabsorptive procedures like gastric bypass, which in turn can cause their quality of life to deteriorate.
Even bariatric doctors admit that WLS does not make the lipedema go away. Many patients have significant weight regain after a few years as the lipedema reasserts itself, so it's hard to say how much long-term help such an approach really gives.
Many supersized women with significant lipo-lymphedema would likely say that such surgery was life-saving and that they would be much worse off had they never had the WLS. That could well be true. On the other hand, it's impossible to know this for sure since they can't go back and see an alternate timeline where the surgery wasn't done.
While it is completely understandable to want to ease some of the health or mobility issues of severe lipedema, that possible benefit must be considered against the real possibility of nutrient deficiencies, internal hernias, neurological issues, hospital readmissions, and other problems that can develop after bariatric surgery, some of which can be life-threatening.
Some feel the possible improvement in mobility and certain health conditions with WLS is well worth the risk of complications and weight regain. Others do not. Whatever choice they make, all deserve to be supported with love and respect.
"Weight Control" for Lipedema
 Even when doctors are realistic about the remote chance of weight loss fixing lipedema, many still strongly encourage dieting behaviors for "weight control" to hopefully prevent additional fat storage.
Even when doctors are realistic about the remote chance of weight loss fixing lipedema, many still strongly encourage dieting behaviors for "weight control" to hopefully prevent additional fat storage.On the surface this seems reasonable, but when you dig a little deeper, there are problems in the assumptions most providers make about lipedema patients, in how this message is brought to patients, and in how lipedema patients are blamed if their lipedema gets worse.
Negative Assumptions About Habits
When morbid obesity (BMI>40 kg/m3 ) co-exists with lipoedema, lifestyle and psychological factors have contributed to the adiposity...If nothing changes in terms of the lifestyle choices of women with lipoedema, there will be no change in her condition either.This sweeping conclusion (citing no evidence, note) speaks to the bias of the providers involved. They believe that a little bit of obesity could just be the lipedema, but if there's a lot of obesity, why then it MUST be because the person overeats and has psychological problems ─ it couldn't possibly be a more severe presentation of lipedema.
A 2008 Paper from a Symposium on lipedema by experts in the field had similar speculations:
It remains unclear whether this increased prevalence of high BMI is part of the disease process, or, is it because the patients are frustrated that despite their diets they cannot reduce the size of their legs, and so they eat even more and gain weight on the trunk as well?A lymphedema treatment clinic that also treats lipedema patients has a similar assumption:
As the majority of patients has already unsuccessfully tried all kinds of diets and weight loss treatments since puberty, in order to change the shape of their legs, they usually end up with a carelessness towards food intake and thus a significant overweight.Augh! Among too many lipedema treatment providers, there are a lot of assumptions about "bad" habits that need to be fixed. While it's true that some fat people do have "bad" habits, many do NOT. Others only develop "bad" habits in response to years of deprivation from dieting.
The truth is that fat people are not all alike. Some have habits that predispose to weight gain, but many do not.
It's time for health professionals to take a more nuanced approach to fat patients, one that individualizes care based on circumstances and history rather than making broad assumptions about a person's habits based only on size, and one which expects reasonable habits rather than unrealistic ones.
Triggering Language and Advice
It's reasonable to encourage healthy eating and regular exercise in hopes of avoiding additional fat storage, but the language used by some providers goes far beyond this. Sometimes it is stringent and fear-mongering. Often it gives conflicting messages.
For example, a 2012 paper on lipedema notes that low-calorie diets rarely help and that many lipedema patients have a long history of dieting and even development of eating-disordered behaviors ─ then turns around and tells doctors to give dietary counseling in order to prevent further weight gain:
Lipedema is frequently misdiagnosed as obesity resulting in disturbed eating behaviour such as anorexia...Lipedema, unlike obesity, hardly ever responds to low-calorie diet. Dietary counselling is advisable as a preventive measure against further weight gain. Medical history of most patients shows that the majority has a history of dieting and exercising without any considerable benefit on the contours and shape of affected limbs.What is the dietary counseling going to be if patients already have a history of dieting and even disturbed eating behavior? How is more dietary counseling going to help? Might it not just make things worse? Why can't they recognize that it is this very dietary counseling that pushes some women into anorexia and disordered eating behaviors?
Experts too often recommend weight control measures that are suspiciously similar to stringent diets with low calories, elimination of entire food groups, and frequent weighing. This, along with scolding for weight gain, can be very traumatizing for some women.
Blame the Victim
Even lipedema doctors that don't push weight loss often promote rigidly restrictive eating plans. They seem to think that if lipedemic women don't diet for weight loss anymore that they will show no restraint and gain hugely. One document (my emphasis) says:
Further fat deposition must be prevented. Weight control is critical.It's understandable to counsel patients not to add extra fat to the lipedemic fat already present. But far too many clinicians seem to assume that any further lipedemic fat gain must be coming from "bad" habits rather than as a result of the lipedema itself.
That's the most troubling part of these "rigorous weight control" messages. They blame the victim rather than the disease if lipedema gets worse.
Some care providers take it one step further. They tell women that lipedema can be kept from worsening if they are only careful enough with weight control and healthy lifestyle. In other words, if it does get worse, the implication is that it's the woman's fault.
This implication is widespread among lipedema providers. One leading lipedema advocate states:
It may be possible to limit the effects of Lipedema, through careful weight management, if diagnosed early enough.The Wikipedia article on lipedema states:
If not kept in check through a healthy lifestyle, lipo-lymphedema can worsen, and patients will become progressively less mobile.Another doctor states:
An unhealthy diet will cause the fat deposits to enlarge. A heart-healthy diet is always advised, and in the early stages of the disease, may help retard its growth.But what evidence do they have for making these statements? None. There are NO studies that suggest that stringent weight control behavior prevents lipedema flares.
Again, doctors just assume that it will. Yet many women with lipedema who are extremely careful with diet and exercise still experience sudden unexplained weight gains. The Fat Disorders Research Society acknowledges this, stating:
Even with strict diet and exercise regimens the disease may progress and further treatments may be necessary.Since hormonal changes or stress seem to be the main trigger of flares, it is dubious that strict weight control alone would prevent its worsening. It's also likely that endocrine issues are involved in lipedema. So why is it only ever about the patient's habits, rather than acknowledging that other factors may also be involved? Far too many providers still assume the problem is originating from the patient's behavior rather than the nature of the disorder itself.
Summary
The best argument for "weight control" is that it might help prevent additional weight gain on the rest of the body, which would help reduce stress on joints and might prevent or lessen some co-morbidities. That indeed would be an advantage.
On the other hand, weight loss research shows chronic "restrained eaters" have a strong tendency towards gaining weight, so weight control attempts could actually backfire. One lipedema expert writes:
A metabolism that is accustomed to a low-calorie diet, as well as the inability to exercise sufficiently because of the joint pain, leads to a cycle of gaining weight and worsening the situation for the joints.This is the typical story of most women with lipedema. They reduce calories and eliminate "bad" food groups, then yo-yo up and down the scale repeatedly. Most regain the weight, many end up heavier than they began, and some develop eating-disordered behaviors and body image issues from years of dieting.
It is distressing, then, that even from lipedema experts, they still get relentless messages about the importance of "rigorous weight control," automatic negative assumptions about their habits, and implicit blame if their lipedema worsens.
Certainly, lipedema patients have responsibility for their own habits and shouldn't increase their weight through carelessness. However, careful attention to diet and exercise doesn't mean that flares and sudden weight gain won't occur.
Lipedema doctors need to watch the negative assumptions they often make about the habits of obese patients, avoid triggering language when talking about nutrition and exercise, and avoid blaming women without knowing the full story.
It's better to ask questions to discern an individual's habits, present multiple options based on those habits, and find the flexibility to work with patients instead of against them. Empower women, don't degrade or shame them. Care providers need to move beyond old weight-biased models of care and find new approaches.
Special Nutritional Approaches

For example, many women with Polycystic Ovarian Syndrome (PCOS) moderate their carb intake to help treat the insulin resistance common to PCOS. Some do it in hopes of losing weight, but many do it simply to lessen symptoms. Many with PCOS have also found that their symptoms are much milder when they are gluten-free.
Similarly, some people with lipedema feel that certain nutritional approaches help reduce lipedema symptoms, or at least keep them from getting worse. Commonly-suggested approaches include anti-inflammatory, low-carb/paleo, or gluten-free diets.
However, it's important to note that NONE of these have actually been tested with lipedema patients in clinical trials.
However, it's important to note that NONE of these have actually been tested with lipedema patients in clinical trials.
You can find many anecdotal reports of people who say they were helped by these nutritional approaches and it's important to take these accounts seriously. However, it can be hard to separate weight loss rhetoric from legitimate nutritional concerns in these accounts, and of course, most are very short-term. When you look at the story of someone who claims weight loss or great improvement with a particular nutritional approach, ask yourself, "How long have they been doing this, and how long has it been maintained?" The success of their story might be considerably different 3-4 years out.
Also watch carefully for hidden food neuroses in these tales of "cures." One site states:
Wheat and sugar are the enemy.Broad statements like this are problematic. There well may be truth in the idea that certain foods are more difficult for people with lipedema, and some may indeed find help in eliminating certain types of food. However, it's SO easy to sucked into a diet mentality that makes certain foods the culprit for every evil and that eliminates large groups of food without any proof that this is helpful.
This is the Just World hypothesis in action, where bad things only happen to those who are doing something "wrong." It's Magical Thinking to believe that if we just eliminate Food X or Y, all our health issues will disappear. Eliminating a particular food group can give people a sense of control over their disease and their future, but it's a slippery slope from there into food neuroses and blaming people for their diseases.
This is territory that must be walked very carefully, if at all.
RAD - Low Inflammation
The biggest trend in nutritional circles lately has been so-called low-inflammation diets. EVERYONE I know right now seems to be an anti-inflammation diet, for every reason under the sun. The sheer trendiness alone of this recommendation suggests caution.
On the other hand, if inflammation really is part of the cause of lipedema, then it makes sense that cutting down on "inflammatory" foods might be helpful. As a result, many lipedema sites strongly promote a "RAD" low-inflammation diet. They contend that wheat/gluten and sugar are the two biggest culprits in increasing inflammation, thus making the lipedema worse. Some also feel that dairy, soy, and possibly legumes are big culprits.
On the other hand, if inflammation really is part of the cause of lipedema, then it makes sense that cutting down on "inflammatory" foods might be helpful. As a result, many lipedema sites strongly promote a "RAD" low-inflammation diet. They contend that wheat/gluten and sugar are the two biggest culprits in increasing inflammation, thus making the lipedema worse. Some also feel that dairy, soy, and possibly legumes are big culprits.
According to one doctor who specializes in treating lipedema, the following points are the "essentials" of the RAD diet:
Lower consumption of pasteurized dairy products, animal protein and fats, simple sugars and carbohydrates (low glycemic), salt and wheat or processed flour products, while enriching the diet with organic fruits, vegetables, whole grains and healthy proteins.
Avoid foods that contain lots of chemicals such as artificial preservatives, flavors, fake sweeteners like aspartame, colors and stabilizers which includes most prepared, packaged and fast foods. A lot of packaged foods have advanced glycation end products or AGEs that can cause damage in the body and increase the risk for diabetes and alzheimers. Cooked foods also have AGEs so raw foodists also support lowering your AGE consumption.
1. Lower fat consumption as fats are absorbed directly into the lymphatics.2. Eat low glycemic index foods to lower insulin levels - insulin makes fat grow.3. Eat lots of fresh vegetables that have enzymes that are absorbed into the lymphatics and in essence "roto-rooter" out the stagnant protein. You can add enzymes with advice from your healthcare provider.4. Lower your salt intake if you are able so you retain less water/fluid.5. Each time we eat we generate inflammation as the lymph system surrounds the gut. Rest the gut by taking a day off and eating liquid type foods such as soups, stews (without meat or at least with pulled meats), smoothies, protein shakes, applesauce, juiced vegetables and fruits.
Many people on the "low-inflammation" diet bandwagon say that they do better when they take gluten (and often all grains) out of the diet completely. Some also eliminate certain fruits and allow only small portions of nuts. Everybody has a slightly different version but these are the basics most commonly seen.
I know of NO studies on whether an anti-inflammatory diet helps lipedema symptoms or not. There are plenty of anecdotal stories of lipedema women who say they have much less serious symptoms and progression when on a RAD diet, but as always one has to remember that anecdotal stories are not proof. This needs to be studied.
Low-Carb/Paleo
Low-carb, low-glycemic, or "paleo" diets are another popular recommendation on lipedema self-help sites. These lower the intake of carbohydrate foods, including grains, fruits, and higher-carb vegetables. Some promote moderate carb intake, while others are more hard-core and seek to nearly eliminate carbs.
Since there is probably a fair amount of crossover between PCOS and lipedema, it's quite possible that lowering carbs might be helpful. If there is an underlying problem with utilizing the body's insulin, and since high insulin levels tend to promote fat storage, then it makes sense to lower your intake of foods that spike insulin levels.
Some people find that they do best taking all grains out of their diet completely, while others do fine with just eliminating gluten and/or one or two other grains that tend to trigger strong insulin reactions (corn or rice are common culprits for many people).
Since there is probably a fair amount of crossover between PCOS and lipedema, it's quite possible that lowering carbs might be helpful. If there is an underlying problem with utilizing the body's insulin, and since high insulin levels tend to promote fat storage, then it makes sense to lower your intake of foods that spike insulin levels.
Some people find that they do best taking all grains out of their diet completely, while others do fine with just eliminating gluten and/or one or two other grains that tend to trigger strong insulin reactions (corn or rice are common culprits for many people).
Hard-core ketogenic paleo/low-carb diets often are difficult to follow long-term. Many people do quite well on them at first but report "crashing" on them at some point. Others do fine on them. If you consider trying one of these, it may be helpful to moderate them a bit. Find the combination that works for you.
"Clean" Eating
It's very trendy right now for people to discuss "clean" eating or eating "real" foods. However, these terms are problematic. They are emotionally-loaded and stigmatizing. They put all kinds of arbitrary labels out there, promoting too much guilt about food.
Foods aren't inherently "good" or "bad," "real" or "unreal;" some are better for your health than others but all have some value. This kind of judgmental terminology is often adopted by people with eating disorders. Food moralizing is a dangerous slippery slope.
Foods aren't inherently "good" or "bad," "real" or "unreal;" some are better for your health than others but all have some value. This kind of judgmental terminology is often adopted by people with eating disorders. Food moralizing is a dangerous slippery slope.
In the context of lipedema, if "clean" eating means eliminating artificial chemicals and additives, then that may be a reasonable goal for someone with lipedema. Cutting down or eliminating processed foods full of additives and preservatives seems unlikely to be harmful and seems likely to be beneficial.
Since lipedema flares are thought to be triggered by estrogen, it seems logical that eliminating possible outside sources of estrogen might be helpful. Therefore, many people with lipedema avoid plastic containers, eat only meat that has been raised organically (no hormones, grass-fed instead of grain-fed), etc.
As long as it's not taken to an extreme, more natural "whole" foods are probably always going to be a good idea and I strongly support people eating that way. But be careful about too much food moralizing; that way lies eating disorders.
Since lipedema flares are thought to be triggered by estrogen, it seems logical that eliminating possible outside sources of estrogen might be helpful. Therefore, many people with lipedema avoid plastic containers, eat only meat that has been raised organically (no hormones, grass-fed instead of grain-fed), etc.
As long as it's not taken to an extreme, more natural "whole" foods are probably always going to be a good idea and I strongly support people eating that way. But be careful about too much food moralizing; that way lies eating disorders.
Summary
It's certainly possible that these special dietary approaches might bring positive effects for some, but pursuing these for a weight control agenda is usually not very successful.
Personally, I do believe that it is helpful to your health to eat more whole foods, cut down on additives, emphasize hormone-free and grass-fed meats, and consume more fruits and vegetables. I believe that many people with PCOS and lipedema do lessen their symptoms somewhat if they cut down on carbs. I know some who swear that going gluten-free really changed their health so I take that possibility seriously too. I'm not putting down the idea that nutrition may be one way to help combat lipedema, nor am I telling people to be careless in their habits.
But I also see an awful lot of Food Moralism and Magical Thinking in these nutritional approaches, and the language used in some of them is way too judgmental. Be very careful about the slippery slope between these and eating disorders.
I'd also point out again that there is NO PROOF that any of these nutritional approaches are helpful to women with lipedema. No one has even done any research to see if they do. Be very careful when reading extravagant claims telling you how you "must" eat for lipedema without any actual data to back up their claims.
If you consider using one of these approaches, use it to see if it affects your symptoms, not as a way to make you skinny, and do it moderately, not in extremes. Experiment and see it if it helps, but use common sense.
Health At Every Size®
 While some women with lipedema still search for the dietary Holy Grail, others have chosen to disengage from dieting and weight management altogether. Some choose a Health At Every Size® approach, focusing on health behaviors rather than a number on a scale.
While some women with lipedema still search for the dietary Holy Grail, others have chosen to disengage from dieting and weight management altogether. Some choose a Health At Every Size® approach, focusing on health behaviors rather than a number on a scale.
Lipedema doctors should understand that many women with long histories of failed dieting have sworn off even the oft-recommended 5-10% weight loss. They feel that even small weight-loss attempts are like playing Russian Roulette with their health; their past experience suggest that even small losses are likely to result in weight gain in the long run.
The choice to opt out of modest weight loss goals or rigid weight control attempts is very threatening to some in the medical community. Many consider this being in a state of denial about obesity, and they believe it is their job to break down this denial and MAKE fat people accept weight control measures like weight loss drugs or bariatric surgery.
There is increasing pressure on primary care providers to be more aggressive in weight control interventions. Some even want to deny healthcare to patients until they lose weight. One lipedema/lymphedema program requires patients to 'contract' for continued care "by exhibiting positive behaviors regarding weight loss, attendance at bariatric support groups, Weight Watchers®, or other beneficial practices." In other words, toe the line on weight control or you won't receive care anymore.
This is a violation of every patient's right to patient autonomy. Patients should ALWAYS have the right to decline treatments they do not want without being punished for this choice. That includes being denied care or access to other treatments. Lipedema care providers must recognize that lipedema patients are within their rights to decline weight loss/control treatment without being harassed about it, PERIOD.
Many lipedema providers falsely assume that if a patient adopts a Health At Every Size® approach, this means they have "given up," will eat uncontrollably, and never exercise. But that is not what HAES® promotes at all. The Association for Health and Size Diversity defines the principles of HAES this way:
You can follow HAES® and still seek to eat more whole foods, lower carbs, and fewer processed foods. A HAES® approach would also promote regular exercise, but in a way that was sustainable and life-enhancing, not extreme. The aim is to improving health and feel better, not to lose weight.
HAES is not "giving up" but rather re-focusing health efforts in a more productive and life-enhancing way. You can read more about the myths and misconceptions people have about HAES® here.
There is no research on a HAES® approach in lipedema patients, just as there is no research on the efficacy of weight loss or weight "control" approaches with lipedema. However, general research on HAES® shows better longer-term health improvements with HAES® than with a weight-loss approach.
There is growing support in the medical community for emphasizing weight stability and weight-inclusive models over weight-loss-at-any-cost approaches. Even the authors of one of the pro-weight control studies above admit that "weight stabilisation is a positive outcome."
For those who want to pursue weight loss or bariatric surgery, of course you have the right to do so. However, those who want to opt out of "weight control" or to pursue a Health At Every Size® approach also have every right to do so, yet some receive harassment or refusal of care for doing so. More lipedema providers and organizations need to recognize that patients have the right to refuse weight treatment. Indeed, for those with a history of eating-disordered behaviors, it may be the only sane option.
Personally, I do believe that it is helpful to your health to eat more whole foods, cut down on additives, emphasize hormone-free and grass-fed meats, and consume more fruits and vegetables. I believe that many people with PCOS and lipedema do lessen their symptoms somewhat if they cut down on carbs. I know some who swear that going gluten-free really changed their health so I take that possibility seriously too. I'm not putting down the idea that nutrition may be one way to help combat lipedema, nor am I telling people to be careless in their habits.
But I also see an awful lot of Food Moralism and Magical Thinking in these nutritional approaches, and the language used in some of them is way too judgmental. Be very careful about the slippery slope between these and eating disorders.
I'd also point out again that there is NO PROOF that any of these nutritional approaches are helpful to women with lipedema. No one has even done any research to see if they do. Be very careful when reading extravagant claims telling you how you "must" eat for lipedema without any actual data to back up their claims.
If you consider using one of these approaches, use it to see if it affects your symptoms, not as a way to make you skinny, and do it moderately, not in extremes. Experiment and see it if it helps, but use common sense.
Health At Every Size®

Lipedema doctors should understand that many women with long histories of failed dieting have sworn off even the oft-recommended 5-10% weight loss. They feel that even small weight-loss attempts are like playing Russian Roulette with their health; their past experience suggest that even small losses are likely to result in weight gain in the long run.
The choice to opt out of modest weight loss goals or rigid weight control attempts is very threatening to some in the medical community. Many consider this being in a state of denial about obesity, and they believe it is their job to break down this denial and MAKE fat people accept weight control measures like weight loss drugs or bariatric surgery.
There is increasing pressure on primary care providers to be more aggressive in weight control interventions. Some even want to deny healthcare to patients until they lose weight. One lipedema/lymphedema program requires patients to 'contract' for continued care "by exhibiting positive behaviors regarding weight loss, attendance at bariatric support groups, Weight Watchers®, or other beneficial practices." In other words, toe the line on weight control or you won't receive care anymore.
This is a violation of every patient's right to patient autonomy. Patients should ALWAYS have the right to decline treatments they do not want without being punished for this choice. That includes being denied care or access to other treatments. Lipedema care providers must recognize that lipedema patients are within their rights to decline weight loss/control treatment without being harassed about it, PERIOD.
Many lipedema providers falsely assume that if a patient adopts a Health At Every Size® approach, this means they have "given up," will eat uncontrollably, and never exercise. But that is not what HAES® promotes at all. The Association for Health and Size Diversity defines the principles of HAES this way:
- Accepting and respecting the diversity of body shapes and sizes
- Recognizing that health and well-being are multi-dimensional and that they include physical, social, spiritual, occupational, emotional, and intellectual aspects
- Promoting all aspects of health and well-being for people of all sizes
- Promoting eating in a manner which balances individual nutritional needs, hunger, satiety, appetite, and pleasure
- Promoting individually appropriate, enjoyable, life-enhancing physical activity, rather than exercise that is focused on a goal of weight loss
You can follow HAES® and still seek to eat more whole foods, lower carbs, and fewer processed foods. A HAES® approach would also promote regular exercise, but in a way that was sustainable and life-enhancing, not extreme. The aim is to improving health and feel better, not to lose weight.
HAES is not "giving up" but rather re-focusing health efforts in a more productive and life-enhancing way. You can read more about the myths and misconceptions people have about HAES® here.
There is no research on a HAES® approach in lipedema patients, just as there is no research on the efficacy of weight loss or weight "control" approaches with lipedema. However, general research on HAES® shows better longer-term health improvements with HAES® than with a weight-loss approach.
There is growing support in the medical community for emphasizing weight stability and weight-inclusive models over weight-loss-at-any-cost approaches. Even the authors of one of the pro-weight control studies above admit that "weight stabilisation is a positive outcome."
For those who want to pursue weight loss or bariatric surgery, of course you have the right to do so. However, those who want to opt out of "weight control" or to pursue a Health At Every Size® approach also have every right to do so, yet some receive harassment or refusal of care for doing so. More lipedema providers and organizations need to recognize that patients have the right to refuse weight treatment. Indeed, for those with a history of eating-disordered behaviors, it may be the only sane option.
Summary of Weight/Nutritional Treatments

However, as always, the choice remains with each person. Some women with lipedema will want to pursue weight loss or bariatric surgery, some will simply try to keep their weight stable, some will try various nutritional approaches, and some will follow Health At Every Size® principles.
Because of the weight bias pervasive in the field, patients need a strong mental filter when perusing lipedema literature. Frankly, there's a lot of nonsense from some researchers about people with lipedema "overeating to console themselves" and a lot of patronizing pseudo-sympathy.
Sadly, many lipedema patients internalize this weight stigma. They beat themselves up for not being able to lose weight, they resort to ever-increasingly restrictive diets, they may develop disordered eating patterns from years of dieting and beat themselves up even more.
After spending most of their lives in this mind-set, it can be difficult giving up the hard-core focus on dieting and weight loss. This can lead to some psychological distress. One lipedema support website notes:
Lipedema people often have difficulty moving beyond the first stages of recovery because we continue to be fixated on changing our bodies in order to fit in with the rest of the world. This has been our goal every waking moment since we were first understood that our bodies do not fit the accepted cultural norm.
...People with lipedema are told our unacceptable appearance is our fault. We have been told all of our lives to fix ourselves so we can fit in with healthy, wholesome, disciplined people or to accept the bullying and name-calling we have earned "one Twinkie at a time."
Lipedema people have spent so much of their lives trying to make themselves physically acceptable with fad diets, exercise equipment, surgeries to reshape us etc, that we cannot stop a lifetime of compulsively trying to change our body shape even after we are told that exercise and diet will not help us. We can't just stop overachieving for the prize "of blending in" especially because one group of professionals tells us there is no cure for lipedema, another professional group promotes surgeries, and still other groups, including psychologists and psychiatrists, haven't even heard of lipedema, and still want to treat us as food addicts.One of the sad facts of lipedema is that we probably will never have a body that looks "normal." Even after bariatric surgery, our bodies will likely still have more fat than average and will remain disproportionate because this is a disease of tissue overgrowth.
...Over the last decade, many lipedema forums, blogs, and self-help groups have addressed lipedema in ways that give us hope. We have learned much and we have created a community of love and support that engages our bodies and spirits. However, the one thing we have not accomplished is healing the shattered psyche of those of us who have been so deeply wounded by society, so estranged and humiliated, that we can't stop the addictive and compulsive survival tactics we unconsciously use in order to be accepted. We can't give up the corporate illusion that we can have normal bodies.
We have to find a way to make peace with our bodies so that we can live happy, fulfilled lives whether or not our bodies ever look "normal." Giving up the body hate and finding body love (or at least what I call "body detente") is the path to happier lives.
Lipedema care providers need to give up the single-minded focus on weight because it is keeping them from focusing on the REAL issues of lipedema. As one person with severe lipo-lymphedema writes:
The diet industrial complex works against those of us with lipedema...to be frank the profit motives are diverting real research in too many areas. I spent 17 years after my huge weight gain in extreme pain and suffering, given false promises of weight loss, and this almost cost me my life due to infections. The diet industry almost led to me dying, as it told me to suppress calories to 'save my life' with answers that simply did not work. Lippys need people willing to work outside the diet industry paradigms and its lies for the betterment of our lives...Lipedema, to be treated in the best way, needs set free from the diet industrial complex. We need thinkers who will think outside the box in the best way to help us, to realize the true endocrine and other issues that lie behind lipedema.Amen to that. Lipedema, as a condition, has been known about for 75 years. Why is it still so hard to get diagnosed? Why don't we have more research on it? Why haven't we made more progress in treating it? Why aren't we doing more to learn about the true underlying causes of lipedema, particularly endocrine issues?
I say it's partly because of the underlying weight bias of the medical world, which wants to see lipedema mainly as a weight issue, and the tremendous profit motives of the diet industrial complex, which only wants to profit from us. Until the medical world gets out of bed with the diet industrial complex, progress on lipedema will remain slow.
It is my strong belief that until we can divorce lipedema from the weight loss industry and eliminate the insidious weight stigma taught in medical education, we won't make much progress towards curing lipedema, let alone finding effective treatments for it.
In the meantime, people with lipedema have to blaze their own trails in finding what works for them.
References and Resources
Resources
*Trigger Warning: Many of these sites are not size-friendly. However, because they also contain valuable information about lipedema and its treatment, they are included here.
- http://www.curelipedema.org/# - Cure Lipedema, lots of info on treatment choices
- http://www.lipomadoc.org/lipedema.html - Website of Karen L. Herbst, PhD, MD, one of the most pre-eminent researchers on lipedema. She is an endocrinologist practicing in Arizona
- http://fatdisorders.org/fat-disorders/lipedema-lipoedema-description - Website of the Fat Disorders Research Society
- http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3309375/ - United States National Library of Medicine, National Institutes of Health
- http://www.nhs.uk/conditions/lipoedema/Pages/Introduction.aspx - United Kingdom's NHS website page on Lipedema
- http://www.hanse-klinik.de/englisch/Lipoedema.pdf - article on lipedema from one of the foremost clinics in Germany that treats lipedema
- http://www.lipv.nl/zslnokycordero.pdf - journal article about lipedema with many pictures
- http://www.lymphedemablog.com/2012/12/13/a-closer-look-at-lipedema-and-the-effects-on-the-lymphatic-system/ - Effect of lipedema on the lymphatic system
- Differential Diagnosis for lipedema vs. lymphedema - how to differentiate these conditions
- http://rlbatesmd.blogspot.com/2010/02/lipedema-lymphedema-lipolymphedema.html - blog entry on lipedema vs. lymphedema, written by a plastic surgeon
- http://www.thelymphoedemacliniclondon.co.uk/pages/treatment-for-lipedema-and-lipo-lymphoedema.php - treatment options for lipedema and lymphedema
- http://blog.wegohealth.com/2014/09/15/the-phases-of-a-lipedema-diagnosis/ - Guide to navigating a lipedema diagnosis, written by Sarah Bramblette, a prominent lipedema activist
- http://www.lipoedemaladies.com/ - U.K. support group for lipedema
- https://www.facebook.com/lilithnixroadtorecovery/posts/537379969717549 - Facebook page of a woman with lipo-lymphedema (this link takes you to her biography and lipedema story)
- http://www.lass.org.au/ - Lipoedema Australian Support Society (LASS)
- http://www.talklipoedema.org/ - U.K. support and information group for lipedema
- https://livingwithlipoedema.wordpress.com/ - a British woman's journey with lipedema, particularly focusing on its emotional effect and the treatments she has tried
- http://www.laurajdavis.com/blog/category/lipolymphedema - one woman's history of lipo-lymphedema, failed attempts at weight loss, and treatment difficulties
Acta Pharmacol Sin. 2012 Feb;33(2):155-72. doi: 10.1038/aps.2011.153. Rare adipose disorders (RADs) masquerading as obesity. Herbst KL. PMID: 22301856
...People with RADs [Rare Adipose Disorders] do not lose SAT [subcutaneous adipose tissue] from caloric limitation and increased energy expenditure alone...
3 comments:
Thank you for this well written, informative post!
Thank you so much for this article. Couldn't have said it better myself. I too have had gastric bypass 13 years ago and suffer from lipo-lymphedema/venous insufficiency/ PCOS/insulin resistance/Hashimotos-Hypothyrodism/severe anemia/estrogen dominance/ malabsorption/secondary hyperaldosteronism/stage 3b-c adrenal fatigue/osteoarthritis and large doses of humiliation and hopelessness. All this was diagnosed on my journey to finding what was really the issue...the lipo-lymphedema. I had no idea it even existed until a few months ago. That is after close to 50 docs/specialist I have seen over the course of 25 years telling me just to lose weight. I became an expert at research and all things medical. Much of this we know is genetic and I have a mother/grandmother/sister/ cousins that all look like me. I was told my veins failed me in my teens maybe earlier. I struggled since puberty with my hormones for sure. Everyone just assumes it was diet related yet my family and I were the healthiest fat people you have ever seen. My mother lived with same complaints and no one would help her. No one is willing to help me. Just visited my first Lipo/Lymph doc and was told to lose 10% of my body fat. I guess they weren't listening when I described my journey, pain and problem with gaining weight with no explanation and how I work my butt off (I wish) at the gym and eat very healthy. I left feeling defeated again. I just want to be healthy, normal, not the biggest person in the room. I want to be seen for my strengths not my (supposed) weakness...I am fat!! I am not unintelligent/incapable/unmotivated...I have a disease...many diseases that make it almost impossible to live the life I know I could/should/would.
I set, on as many supplements as I need to keep my nutrition normal, help my inflammation and my immune system. I have no pouch from bypass so basically have a sleeve and am slowly dying anyway from malabsorption/malnutrition. I do not absorb fats so how can I go on the low fat diet suggested by so many...we do NEED fat to live. I can only eat so much...I am not one of those gastric bypass patients that went back to old habits. I eat around 100g of protein a day and still have borderline low protein...how can I go NO beef/dairy (it's grass fed/organic anyway)? I need those things just to get me through day to day. I have to be low carb or I dump. I can not change anything there. They say eat more fruits/veggies but I have very little HCl so can not digest well even with supplements and get very gassy...ever felt like you were being cut in half with pain? I have numerous times because I ate a normal portion of fruits/veggies...they turn to gas because of the fiber. It is pain you will never forget and takes hours to go away. I too have felt better with low/no gluten however, that means no fiber for me because of the afore mentioned so now what? I barely get to eat much of anything anyway. I dare any of those above mentioned 50 docs to try to eat like me for a week and see how they feel.
I don't know what the future holds but I am focused on quality of life at this point and I am only 40 years old. I know I will not see 60 years old most likely. My body already feels like it is 80 years old and there is no cure to what I have...lipo-lymphedema and then some.
I can say self management is the only way, there are approximately 15 to 20% of us who are of normal weight as a small but significant minority there is a complete lack of information for us maybe because the powers that be can't see beyond calorie restriction
Post a Comment